


In 2008, New York City Planned to Move, Store, and Dispose of Tens of Thousands of Bodies due to H5N1

I’m working to expose the truth of the “death spike” in New York. In Part One of what I call Cuomo’s Death Spike, I reported the critical shift in PCR testing from the US CDC to the State of New York, which gave New York to form their alibi for murders by medical professionals by protocols and countermeasures.
A Time article published March 31, 2020, reported that the plans to deal with tens of thousands of bodies had already been laid in 2008. I’ll start with some of the reporting from this article, then get into the Plan from the NYC OCME (Office of Chief Medical Examiner).
Time: ‘I Still Can’t Believe What I’m Seeing.’ What It’s Like to Live Across the Street From a Temporary Morgue During the Coronavirus Outbreak
Under the New York City medical examiner’s protocols for a pandemic, the deployment of temporary morgues becomes necessary when the death toll tops 200 per day, overwhelming the capacity of hospitals to store bodies safely. New York City passed that threshold last week, triggering a new “mobilization level” in the city—the third level on a scale of six—according to a copy of the chief medical examiner’s pandemic “surge plan” for handling the dead, which Worthy-Davis shared with TIME.
Drafted in 2008 to prepare for a devastating flu pandemic, the plan envisions far more dramatic measures of “mass fatality management” if the virus continues to spread. Officials at Rikers Island, the city’s main jail, could put inmates to work burying some of the dead in the city-run public cemetery on Hart Island, the plan states. Under the current level of mobilization, the city must also draw up contracts with cemeteries that can accommodate temporary mass graves, which the plan describes in jarring detail: “Ten bodies in caskets are placed lengthwise in a long narrow section in the ground.”
The burial plans were executed to the letter beginning in early April 2020. It looks like they stacked the pine boxes 5 high and 2 wide on Hart Island. NPR reported the mass burials on Hart Island using prison labor from Rikers Island on April 10, 2020:
NPR: Burials On New York Island Are Not New, But Are Increasing During Pandemic

Later in the summer of 2021, as 750 bodies still remained in freezer trucks, PIX11 News reported that the Hebrew Free Burial Association “saved 523 people from a mass grave in 2020.” Sadly, one of the Jewish victims of the Hospital Holocaust saved from burial in a mass grave was a survivor of the Nazi Holocaust in Germany.
The following are some excerpts from New York City’s Medical Examiner’s “Surge Plan” for managing Hospital Deaths, October 2008:
The City of New York Office of Chief Medical Examiner: Pandemic Influenza Surge Plan For Managing In-and-Out-of-Hospital Deaths
The World Health Organization predicted an H5N1 P(l)andemic sometime prior to New York City’s Death Management Plan in 2008.
The World Health Organization (WHO) suspects the H5N1 virus will be the next virus to cause a PI outbreak. The H5N1 avian influenza strain has currently caused human illness in Asia, Africa and the Middle East. To date, over 300 human cases of H5N1 have been reported, with a greater than 60% fatality rate in humans. Most of these cases, however, were due to direct or indirect exposure to infected poultry and were not the result of human-to-human transmission. While there is currently no imminent threat of a pandemic being caused by H5N1 or any other novel influenza strain, the WHO is concerned about the possibility that this H5N1 viral strain may mutate to a form that is more easily transmittable from person to person and thus cause a PI outbreak. Recognizing the possibility of a future PI outbreak, key New York City (NYC) government and private sector agencies have conducted planning sessions and developed response strategies both for managing the influx of medical patients and for handling the fatalities. The City of New York Office of Chief Medical Examiner (OCME), as part of the NYC Department of Health and Mental Hygiene (DOHMH), has developed an annex to its City of New York All Hazards Mass Fatality Management Plan. This annex, entitled “The City of New York Pandemic Influenza Plan For Managing In- and Out-of-Hospital Deaths,” is designed to outline the OCME’s planned response to a naturally occurring influenza outbreak that results in many deaths.
Funding for New York City’s Plan was provided by ASPR.
Grant funding provided by the Office of the Assistant Secretary for Preparedness and Response (ASPR) was used to develop this plan, via Grant 1 U3RHS0756-01-00. Its contents are solely the responsibility of the authors and do not necessarily represent the official views of ASPR.
Aside: ASPR is a government agency within the Department of Health and Human Services.
Wikipedia: Under the Pandemic and All Hazards Preparedness Act of 2006 109–417 (text) (PDF)), HHS is the lead agency for the National Response Framework (NRF) for Emergency Support Function 8 (ESF-8). The Secretary of HHS delegates to ASPR the leadership role for all health and medical services support functions in a health emergency or public health event.
New York City’s Plan has an image of U.S. Department of Health and Human Services Secretatary Michael Leavitt with the caption “It’s not a matter of if, but when.” The link to the video in the .pdf no longer functions.
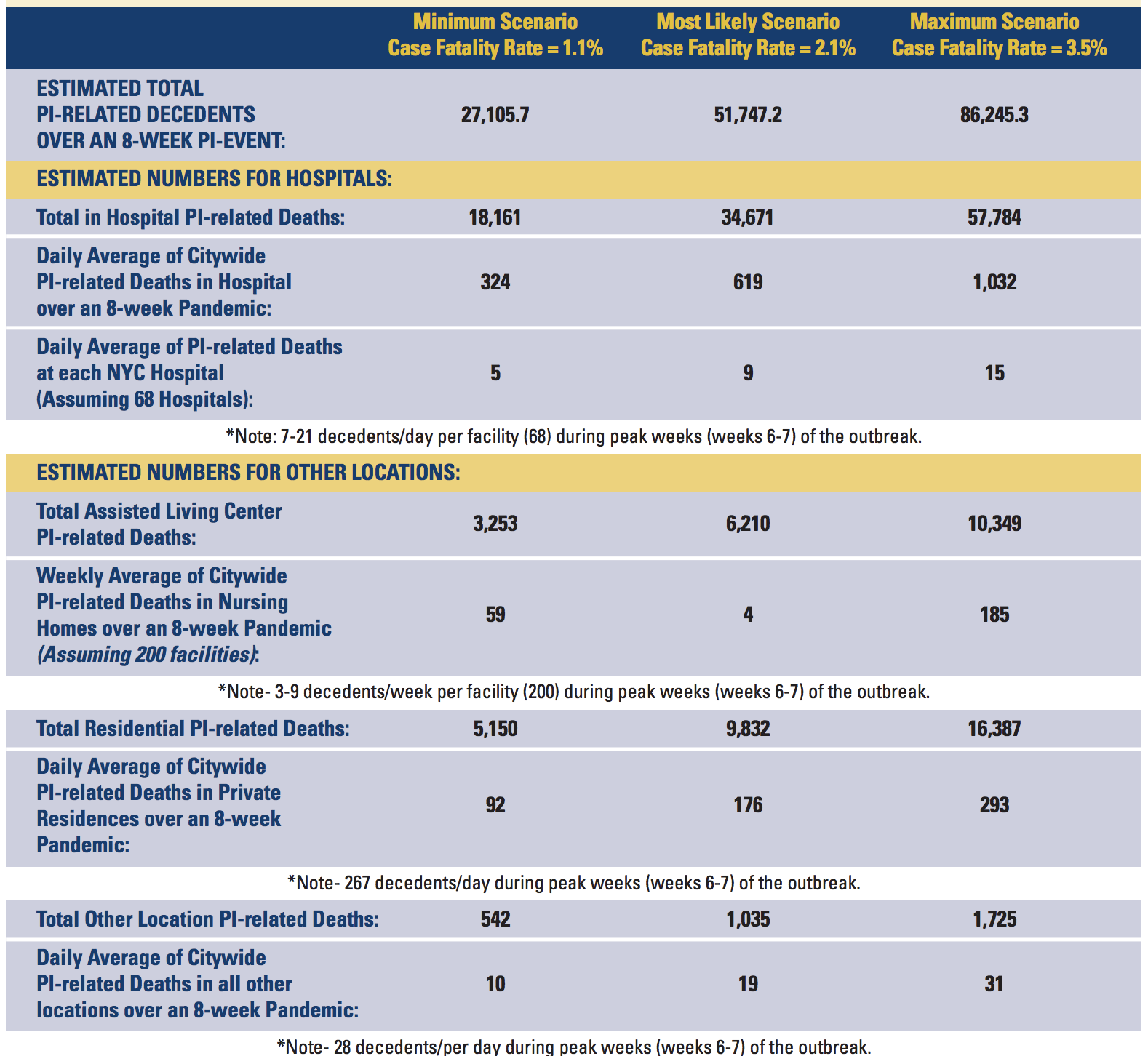
New York City estimated 51,747.2 deaths as a “most likely scenario” from H5N1 within a range of 27,015.7 on the low side and 96,245.3 on the high side.
To understand the magnitude of a PI event in NYC, the OCME worked with the Department of Health and Mental Hygiene (DOHMH) to estimate the number of decedents. Based on NYC’s estimated population of 8.2 million (which increases to about 8.7 million during business hours), an estimated infection rate of 25-35% of the population and an associated mortality rate of 2.1% of the population infected,4 the OCME must be prepared to manage 51,747 additional decedents. This is more than twice the number of decedents that the OCME processes annually and it must be prepared to manage this influx during an 8-week period. (See figure on pg. 7 for other fatality rate calculations.) These deaths will occur over the entire 303 square miles that make up New York City’s five boroughs.
They will occur at private residences, at NYC’s 68 hospitals, its more than 200 nursing/assisted living homes, its 400-plus clinics and physicians’ offices and at the 11 correctional health care facilities (HCFs) associated with NYC’s prisons.
They estimated that the “most likely” death scenario was 34,671 deaths in hospitals, 6,210 deaths in assisted living facilities, and 9,832 residential deaths.
The City outlined a need to deal with the large numbers of bodies in a respectful manner- their “new normal.”
A PI event will be particularly challenging due to the potential for tens-of-thousands to hundreds-of-thousands of deaths to occur. The private sector could be left with the responsibility to deal with decedents, as most naturally occurring deaths never come under the OCME’s jurisdiction. The magnitude of a PI event, however, would demand a response from the OCME, to assist both City health care facilities (HCFs) and to support private sector funeral directors, cemetery/crematorium owners and religious communities. In such an instance, the OCME’s goal would be to provide a service to the community, so that decedents could be cared for respectfully even during a devastating disaster likely to create a “new normal” regarding how human remains are processed.
OVERVIEW
The OCME will arrange to have Body Collection Points (BCPs) placed at eligible HCFs, to temporarily increase their storage capacity. These refrigerated units can hold approximately 9-44 bodies. The BCPs placed at HCFs should be used for all decedents having died from natural causes, including both PI and non-PI related deaths. It is likely a significant number of decedents will not have a known identity; although these deaths would normally be categorized as a medical examiner (ME) case, the OCME has determined they should be placed in the BCP. The BCP should not, however, be used for any other cases requiring ME investigation (e.g., therapeutic complications, violent deaths including homicides, suicides and accidents and all custody deaths).
OPERATIONAL STRATEGIES

The OCME will expand its morgue operations by decentralizing its management approach, giving Borough (B)-OCMEs command and control of decedent operations in their area. B-OCMEs will enhance their current operations by increasing existing storage space, modifying staff schedules and expanding their capability with off-site morgues (OSM). These OSMs will be established in association with B-OCME morgues experiencing an increase in decedents. Primarily, OSMs will be used to process PI cases that require identification and PI evaluation. This will allow B-OCME facilities to process both PI and non-PI cases that require an extensive evaluation and/or autopsy.
This text below might describe a good basis for some FOIA requests on the numbers of bodies handled during the still-ongoing Hospitals Holocaust (COVID Plandemic) in New York:
During a PI event, the Office of Vital Records will coordinate with OCME to establish a Distributed Death Registration Process (DDRP) at each B-OCME and OSM. This method entails the use of the Electronic Death Registration System (EDRS) to facilitate the registering of death certificates and the issuance of burial/cremation/transport permits at remote locations. Funeral directors will be able to retrieve the registered death certificate and associated permits in the same location as the body. This will avoid overwhelming the City’s Central Burial Desk.
They planned to use refrigerated storage, of course.
The first tier requires the use of refrigerated RSFs, placed at B-OCME locations. These RSFs can be organized to facilitate easy storage and retrieval of bodies, since most PI cases will have known identities, as well as medically established cause and manner of death identified on signed death certificates. These cases can be fast tracked, since they are only being held until the private sector can manage final disposition.
Bloomberg reported on March 25, 2020, that New York City had purchased 45 refrigerator trailers.
Multiple outlets reported that FEMA was sending an additional 85 refrigerated trailers in late March, 2020. The exact date of the first media report of FEMA sending the 85 refrigerated trailers is a bit unclear. Jalopnik reported on March 26, 2020 that “the New York Times reports that the state has requested 85 refrigerated trailers from FEMA to house the anticipated number of bodies as a result of COVID-19.” Oddly, the link to the New York Times article does not include any information on FEMA or the refrigerated trailers. The New York Times article was published on March 25, 2020 and was edited on April 14, 2020 to remove the reference.
So that’s 130 refrigerated trailers ordered by March 25, 2020, at the latest. These are all 53-foot long trailers in the multiple pictures that I have seen of them.

NYC planned to increase cremations.
Tier one may also require increasing NYC’s cremation capacity. The OEM, working with the OCME and the DEP, may request modifying existing restrictions, through a Mayoral Emergency Order, to accommodate a large influx of voluntary cremation requests.
NYC determined the capacity of crematoria in their five boroughs and determined that the NYC Deparment of Environmental Protection would need to ease restrictions.
Within the five boroughs, four crematoria exist having a total of 17 retorts. At present, only three retorts function, processing fewer than two bodies per day. Due to restrictions placed on crematoria owners by the NYC Department of Environmental Protection, crematorium owners do not run their operations near capacity; thus it is possible to accommodate large influx of decedents if these regulations were modified. For example, crematoria only operate six days a week and only during specific business hours; one cremation usually takes approximately 3-4 hours.
Aside: A large amount of cremations also occurred in the Hospitals Holocaust, which is very similar to Auschwitz in the Nazi Holocaust. 1940-1943: “Crematorium I operated [at Auschwitz] from August 15, 1940 until July 1943. According to calculations by the German authorities, 340 corpses could be burned every 24 hours after the installation of the three furnaces.”
From Time, May 21, 2020:
‘We Do This for the Living.’ Inside New York’s Citywide Effort to Bury Its Dead
Faced with limits on funeral attendance and social-distancing restrictions at grave sites, many families are opting instead for cremation. At Green-Wood, the number has tripled to more than 150 each week. New York State regulators realized in early April that demand for cremations would rise, so they loosened restrictions to allow crematories to operate around the clock. All five of Green-Wood’s cremation ovens now burn up to 1,800°F for 16 hours a day. (The remaining eight hours are needed for recovery time.) The overuse has caused two of the ovens to break.
All four city crematories have backlogs stretching to a month. None has ever had a wait list before. Funeral directors have resorted to driving bodies to crematories in Vermont, Pennsylvania, Connecticut—anywhere that’s not overwhelmed.
And again, New York City planned mass burials on Hart Island with prison labor.
When RSFs are at or near capacity and NYC does not have access to additional cold storage units, the OCME will direct temporary interment at the Hart Island Cemetery, managed by the Department of Correction (DOC), as its second tier approach. As of 2007, the DOC reported that Hart Island has two prepared sites able to accommodate 19,200 decedents and an additional undeveloped site to support future interments. Until that site is cleared, however, the DOC cannot estimate its capacity.
New York City also they said they could use the Deparment of Defense’s methods to handle bodies, but didn’t specify what those methods were, or at least the language is unclear to me.
The third tier requires the City, coordinating with the OCME, to establish contracts with public and/or private cemeteries capable of accommodating temporary interment for numerous decedents. Contracts must specify the cemetery’s services, including in-the-ground interment, tracking, case record management and the ability to disinter. Contracts may also recommend that cemeteries utilize the Department of Defense’s (DOD’s) temporary mass interment method. This method avoids stacking decedents and minimizes hand digging as part of initial interment and disinterment. (Ten bodies in caskets are placed lengthwise in a long narrow section in the ground. The foot end of one casket is placed in close proximity to the head end of the next casket.)
NYC planned to use “three-tiered racks” in their “Logistics” section.
OEM Logistics The OCME may require OEM Logistics support to enhance their facilities and obtain additional supplies, equipment and personnel. The following list identifies the major facility, equipment and supply requirements associated with specific OCME capabilities as well as skilled personnel capable of supporting OCME operations: • B-OCMEs − Equipment—Storage enhancement devices such as three-tier racks
And yes, they built 3-tiered racks for bodies in New York in the Plandemic. The image below is from the Time’s I Still Can’t Believe What I’m Seeing.’ What It’s Like to Live Across the Street From a Temporary Morgue During the Coronavirus Outbreak.
Workers build shelves for a makeshift morgue outside Wyckoff Heights Medical Center in Brooklyn, New York, on March 30, as seen from an apartment building across the street.

There’s plenty more I could report, but you get the picture. The most important thing in my opinion is to read, share and discuss the Pandemic Influenza Surge Plan For Managing In-and-Out-of-Hospital Deaths, which I only discovered recently. It seems like a Plan that should be discussed more in the context of the “death spike” in New York in Spring 2020.
Charles Wright
When that many people die so swiftly, it's NEVER from "natural" causes, unless there's a massive earthquake, hurricane, fire, etc.. But these days, we also know they can do these things to us as well.
I suppose you would think it’s real if all you did is actually watch the news. Investigative journalism reveals it’s all
Lies. Hollywood to fool the uneducated. First of all these viruses are all computer simulations never proven to exist beyond the program. Research it. Secondly. Walk over and visit these graves sites they are empty. All media is owned by these controlling families. Fear is used to shut down critical thought. And PCR is a bs test. That can be falsified. It was never meant to dx.