


On Steve Kirsch, Bill Gates, Jeff Rothschild, Gilead Sciences, Remdesivir, and "Victoria Cyanide."

In February 2021, Victoria Yan and Florian Muller published a paper titled: “Remdesivir for COVID-19: Why Not Dose Higher?”

They thanked Steve Kirsch for funding them.

By this time in early 2021, Yan, Muller and Kirsch should all have had plenty of evidence that Remdesivir was ineffective and deadly. In fact, Yan and Muller argued that the dosing of Remdesivir was ineffective and unsafe. Instead of calling for an immediate suspension of the Emergency Use Authorization of Remdesivir, however, they advocated for a “front loading” strategy of Remdesivir.
Comparing the magnitude of hepatotoxicity in healthy participants ties transaminase elevations to total dose exposure (Table 2); hepatotoxicity was not observed in the 225-mg single-dose cohort (10). For reference, the recommended dosage (200-mg loading dose, 100-mg maintenance) results in total doses of 600 mg (5 days) and 1,100 mg (10 days), which fall below the threshold for hepatotoxicity (1,050 to 2,100 mg). If viral suppression is a Cmax (maximum concentration)-driven effect and the degree of hepatotoxicity relates to cumulative exposure, then it may be possible to compress the dosing schedule to enable higher dosing while maintaining the same cumulative dose. For instance, a 300-mg loading dose with 200-mg maintenance for 5 days yields a cumulative dose of 1,100 mg.
Worth a try, right? No, it isn’t. They’re gambling with a very deadly substance with other people’s lives.
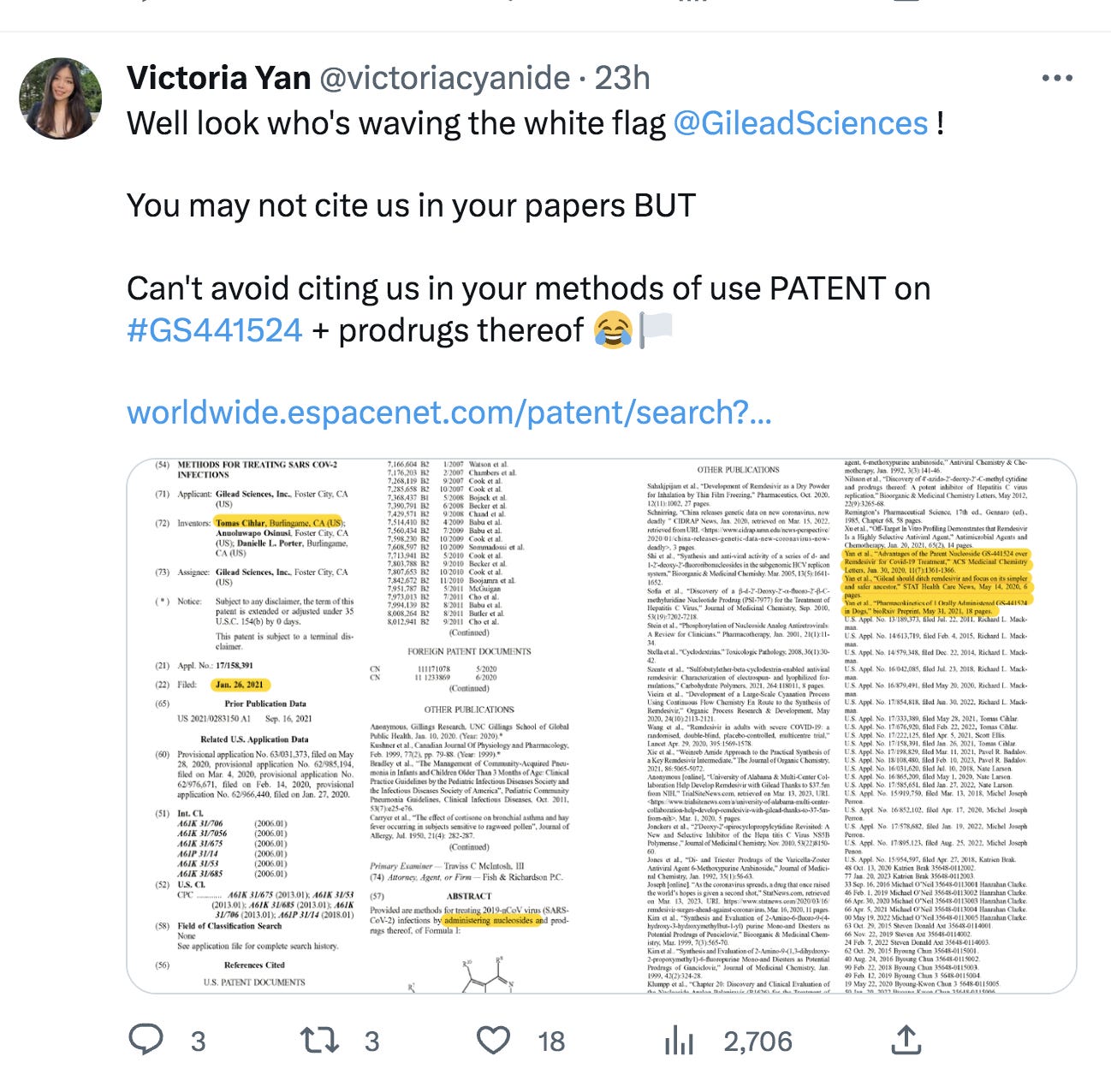
Stew Peters interviewed Thomas Baine on cyanide like properties in the composition of Remdesivir. Victoria Yan chooses to use the name “victoriacyanide” on twitter.

I’m going to say that the cyanide name Yan chose is not a coincidence to the cyanide-like properties of Remdesivir. I’ve asked Victoria Yan on Twitter to explain why she chose to used the name victoriacyanide. She hasn’t commented. She really seems to like cyanide, or be interested in cyandie, or something. In Yan and Muller’s paper, Remdesivir for COVID-19: Why Not Dose Higher?, Yan actually used the email address of “victoriacyanide@gmail.com” as you can see below.

How did Steve Kirsch get himself mixed up in all this, with a lady who calls herself victoria cyanide?
The Kirsch Foundation bragged that it was #8 on the “Philanthropists” list in 1999, with the Bill and Melinda Gates Foundation in the #1 spot.
Kirsch started his COVID-19 Early Treatment Fund (CETF) around March or April of 2020. Treatearly.org: “On Sunday, March 7th, 60 Minutes featured CETF in a story about using Fluvoxamine as an early treatment for COVID-19.” PR Newswire: “The COVID-19 Early Treatment Fund (CETF) …. is administered by Rockefeller Philanthropy Advisors, a 501(c)(3) organization.”
By May 2020, Kirsch, Yan, and Muller were communicating with Gilead Sciences. How Kirsch, Yan, and Muller all got together, and Kirsch came to fund them, I don’t know. Victoria Yan wrote a letter to Chemical and Engineering News describing their conversations with Gilead.
LETTERS TO THE EDITOR (Chemical and Engineering News). June 18, 2021. Victoria Yan, Houston
In May 2020, Florian Muller, Steve Kirsch, the scientific advisers at the COVID-19 Early Treatment Fund, and I communicated to the Gilead leadership the several advantages that GS-441524 possesses over remdesivir. These include being orally administrable; significantly safer, which enables up dosing; and easier to synthesize. Despite presenting compelling data, we encountered an unwillingness to proceed with GS-441524 development. We recognize that, at the start of the pandemic, remdesivir was better poised for repurposing given prior clinical experience. However, it is unclear why prompt development of GS-441524 could not be initiated once remdesivir’s marginal clinical efficacy became evident—especially considering the wealth of data on GS-441524 included in remdesivir’s new drug application to the US Food and Drug Administration. Gilead cites suboptimal bioavailability of GS-441524 in nonhuman primates as a deterrent, yet drugs of the same class demonstrating nonideal bioavailability, such as acyclovir, ultimately demonstrated sufficient absorption to yield clinically meaningful activity in humans. In fact (though anecdotal), I demonstrated acceptable bioavailability of GS-441524 in a pilot self-investigation, in which three times daily dosing of 750 mg easily and safely achieves plasma concentrations exceeding that required to eradicate SARS-CoV-2 in vitro. Had development begun in May 2020, GS-441524 would be in Phase 3 trials today—resembling molnupiravir’s development.
Yan and Muller have definitely been pushing for GS-441524 for some time. Maybe GS-441524 is safer than Remdesivir, and maybe it isn’t. By now though, with all the deaths from Remdesivir, these people should be calling for the criminal prosecutions and the death penalty for Gilead, FDA, and NIAID employees. Instead they are advocating for another Gilead product. Based on many of their publications and tweets, Yan and Muller are pushing Gilead to get a patent for GS-441524 for COVID.
I imagine they expect something for it. I don’t like it one bit. I intend to look into the Gilead patents more in depth later.
In the May 2020 communication period, it also seems likely that the CETF was trying to acquire some Remdesivir supply for testing. On June 2, 2020, Forbes wrote that “(CETF) is also raising funds to support COVID-related trials of remdesivir.” If they ever conducted a test specifically of Remdesivir, I haven’t seen it yet. But they used it for test control comparison.
Remdesivir makes a great control group for testing if you want to look good by comparison. You could go to Robert Malone’s farm in Virginia, scoop up some horseshit, compare it to Remdesivir as a “standard of care,” and say that horseshit cured COVID. (In fact that’s what the Famotidine trials at Northwell did. Not horseshit, but Famotidine + Remdesivir was compared to Remdesivir). If anything, Famotidine is a partial antidote to Remdesivir. “COVID” wasn’t killing the patients in the Northwell Famotidine trials. That’s literally the level of statistics that are used to approve medications today. Obvious lies. The FDA is sadistic and evil. Their goals are to murder and create profit.
On April 29, 2020, Anthony Fauci stopped his Remdesivir trials early. These Remdesivir trials killed the hell out of people. 8% died in the Remdesivir group, and 11.6% died in the placebo group. I’m not sure how they killed so many in the placebo group to make Remdesivir look better by comparison, but they did it. It was probably ventilators and opioids.

On May 1, the FDA issued an EUA for Remdesivir, despite the horrifying death rates. And again, in May 2020, Kirsch, Yan and Muller began talking to Gilead. I’m sure it had something to do with recent grant of the EUA for Remdesivir.
On May 10, 2020, Steve Kirsch tweeted this:

May 10: “Peginterferon lambda is 100x better than remdesivir.” Yeah well, what isn’t 100x better than Remdesivir? Kirsch knew Remdesivir was poison at this point, because he said lambda had “no toxicity” (as opposed to Remdesivir).
That same day, May 10, 2020, Stanford University began Peginterferon lambda trials for COVID. The Mercury News reported the Stanford lambda study: Stanford’s new coronavirus treatment approach: Hit hard — and early.
Stanford is recruiting newly-infected people in hopes of reaching 120 volunteers by Memorial Day. Volunteers must be treated within three days of being tested. The drug is given as one shot — less painful than a flu vaccine — which lasts for days. Patients are seen nine times. In addition to Stanford, New York City’s Mount Sinai Medical Center is also conducting a trial.
Currently, the only proven medication for coronavirus – remdesivir – is given intravenously to patients in hospitals after people get sick enough to be admitted. Even then, its benefit is only modest. People still die. …
At 62, Kirsch has diabetes, high blood pressure and is immunocompromised. The Massachusetts Institute of Technology-trained engineer, who has founded seven companies and invented an early version of the optical mouse, cannot risk going out into the world until there are better early treatments, or a vaccine.
“Trump can open up the country as fast as he wants, but I am still locked down,” he said. “If I get the virus, there is nothing proven today to reduce my chance of death. I’d like to be able to go out and do things. But the risk is too great.”
The two-week-old fund, seeded by Kirsch’s $1 million gift and seeking new donors, aims to find the quickest, safest and lowest cost way to repurpose drugs to dramatically reduce hospitalization rates.
I can’t tell if the Stanford lambda trials used Remdesivir or not. It says they compared Lambda + standard of care to Placebo + standard of care. What was the standard or care?

(The Mount Sinai Lambda trials in New York were withdrawn without posting results. I don’t think CETF was funding them).
Camostat mesilate trials in Denmark, however, definitely used Remdesivir. These trials used Remdesivir in both the control and test groups, as a matter of fact.
“Remdesivir was administered to 96 participants; 64 (47%) in the camostat group and 32 (47%) in the placebo group.”
That study had some very high death rates, as you would expect. CETF was reported to be funding camostat mesilate trials in Denmark. A CETF webpage also says that the CETF funded camostat mesilate trials in Denmark. I assume these trials that used the toxin Remdesivir in Denmark were the same trials funded by CETF.
Kirsch said on August 3, 2020 that “clinical trials are starting at Gilead for an inhaled version of Remdesivir, which looks promising.”
August 3, 2020. Millions Still Needed To Fund COVID-19 Early Treatment Research
"I tend to gravitate toward these more difficult problems, that when you solve them, they make a significant impact," he told KCBS Radio on Monday's "Ask An Expert" segment. "I put in a million dollars of my own money and raised another two million from other people like Jeff Skoll, Elon Musk and others."
Kirsch said CETF needs $17 million more to test the eight different approaches it has identified for treatment. He added that clinical trials are starting at Gilead for an inhaled version of Remdesivir, which looks promising.
It’s unclear to me how Kirsch’s CETF is set up, who all contributes to it, or who is deciding what should be tested. Steve Kirsch wrote the following in an editorial to the Mercury News on May 20, 2020.
Opinion: How America can beat the coronavirus and save lives.

He mentioned that the top 5 contenders that “researchers have identified” were “remdesivir, peginterferon lambda, camostat, favipiravir, and niclosamide.” What researchers? Kirsch also said that Bill Gates and Jeff Rothschild were contributing millions to fund these trials, but that more funding was needed, so he created the CETF to raise that funding. Kirsch wrote on Substack: “Bill Gates is super impressive. I’ve known him for over 40 years.”
Like Bill Gates and Jeff Rothschild don’t have that kind of money. So they need a few million, eh Steve? (Jeff Rothschild is a billionaire and a major funder of Stanford “medical research”). What they needed was a better front man, one that didn’t have such a bad reputation. Enter Steve Kirsch.
If you want to destroy your reputation as a “philanthropist,” however, the only way to do it faster than with vaccines is with Remdesivir. It doesn’t matter how much you implore your old friend to come to his senses on the COVID vaccine death program (that was set up by Remdesivir).
Debate that.
Charles Wright
P.S. thanks to Dr SDRK for much of the research in this article.

Thanks for researching & posting all this. Seems as though we are quickly running out of good guys in this fiasco.
The really sad part of this is that hospitals have had protocols in place and Doctors have treated viral pneumonia for decades. That's all this was. Successfully in most cases unless the patient was old, frail with numerous medical issues. If the FDA and CDC had left them alone to treat them as usual I bet the death count would have been much lower. But then there wouldn't have been millions to be made by Big Pharma, and all the other corrupt players involved in this scheme. They also couldn't have forced the lock downs, the panic and fear and hurt President Trump. None of this needed to happen. None of it. I have yet to find anyone who died of Covid at home or knows anyone who did. If people were dying of the disease, why is that? Why weren't the homeless dropping like flies in the street? All the deaths occurred in the hospital. It wasn't the disease, it was the treatment. Where are the stories of people who say "I wish I had gotten my loved one to the hospital so they could have given them Remdesivir and a ventilator and saved their life?"