It’s the same story everywhere. Medical professionals killed their patients with ventilators and drugs all over the world, and the government agencies of the world, the media, and the scientific ad medical professionals all blamed it on a virus.
The first cases of “COVID” in Italy were tied directly to Wuhan, China, in a couple that returned from Wuhan to Italy on January 23, 2020. In the United States, the first case was also tied to Wuhan, with the unidentified “Snohomish County man.”
The “COVID” death bomb didn’t go off in Washington though, other than one confined mass murder event at a nursing home, however. It skipped all the way across the United States to New York and went off after the CDC allowed New York to conduct its own PCR testing on February 28, 2020. New York tried their best to make the bomb go off earlier in February, but the CDC did not cooperated and returned 100% negative results to New York based on their contact tracing of people returning to New York from China, Italy, and elsewhere.
To understand PCR testing, one must learn from Dr. Kary Mullis posthumously, because Mullis passed away under questionable circumstances in 2019. Paraphrasing Mullis, he said that a PCR test tells you something, but that Doctors have absolutely no clue what it means. A PCR simply amplfies tiny molecules in the human body to a point where they are measurable. What are the molecules? Where did they come from? What are their roles in the human body? They have no clue and make no effort to find out.
If the PCR tests came back positive, medical professionals killed their patients with protocols, simple as that. They don’t think for themselves. They follow orders. Even if they observe deaths over and over from their “treatments,” they don’t care. If their jobs depend on killing, they kill. The hospital’s legal team will protect them if need be. Some of them more experienced with ventilators, like Dr. Pierre Kory, knew good and well what the results would be beforehand.
If the CDC was using an accurate PCR test that searched for molecules at several unique locations in the SARS-CoV-2 sequence, those tests would have naturally returned negative results, because the sequence never existed in a human in the first place.
In China, the “Wuhan Seafood Market Virus” sequence was reportedly created by taking a sample of all materials in lung fluid, breaking the entire spectrum of fluids down into tiny pieces called “contigs,” and reassembling the contigs into the closest match possible of other coronavirus sequences. In turn, these other prexisting “coronavirus” sequences which later generated the “Wuhan Seafood Virus” were based upon were created by the same fraudulent methods.
Many of these tiny molecules in the lung fluid samples from Wuhan were so common that even goats and fruit tested positive for “COVID” in Tanzania, after they attached human names to the samples to check if the labs testing for “COVID” were trustworthy.
Upon information and belief, the CDC must have been using an accurate PCR test in February 2020, actually based on key unique locations of the sequence. The CDC returned 100% negative results to New York in February 2020 as the “pandemic” (ventilators and drugs) raged in Italy and China. New York later lobbied to use one that would return positive results, and received permission on February 28, 2020, which allowed the ICU bomb to go off in New York in early March after a delay.
The rest of this article is simply open source reporting that Italy killed their patients with ventilators. Again, simple as that. The reporting of course only shows a “correlation” between the deaths and the use of ventilators, although in hindsight, any idiot can see what happened.
First two confirmed cases of coronavirus also in Italy. This was announced on Thursday evening by Prime Minister Giuseppe Conte during a press conference. They are two Chinese tourists, already hospitalized in isolation at the Spallanzani hospital in the capital: they are defined as "in good health". The Conte government, meanwhile, has proclaimed a national health emergency for six months and has decided to suspend air flights to and from China. Here are all the updates in the article with the latest developments.
The two tourists were rescued in the Grand Hotel Palatino in Via Cavour, in Rome. They had been in Italy since January 23. The rooms in which the husband and wife stayed were sealed to allow the ASL to carry out the decontamination. The couple is originally from the province of Wuhan. Husband and wife, 67 and 66 years old, arrived in Rome after a tour of other Italian cities. The two felt ill on Thursday and, given the symptoms, were taken care of by 118 staff and hospitalized at Spallanzani.
In February, Sendach and coleagues joined a call with hospital leaders in Italy when the Italians were going through hell: “They told us that it’s going to trickle and then, by the second week, it’s going to just overwhelm you.” They told us it’s not exclusively older people; that they were not sure why people crashed so suddenly.
Northwell in New York had already cleared out their hospitals by February, but they couldn’t start their kill program until the positive PCR test program was in place.
At the time of writing, the whole of Italy is under quarantine measures as it battles to contain an epidemic that has infected more than 7,000 people and killed at least 463 in the country. According to the WHO, 80% of those infected have mild symptoms - but the minority who require hospitalization could be enough to overwhelm healthcare systems if the epidemic spreads.
Dr Daniele Macchini, an Intensive Care Unit physician in Bergamo, a city near Milan, shared his experience of working in a hospital where exhausted staff battle to save patients. His Facebook post was picked up in an Italian newspaper and translated on Twitter by Dr Silvia Stringhini, an epidemiologist and researcher based at the Geneva University's Institute of Global Health.
"I myself watched with some amazement the reorganization of the entire hospital in the past week, when our current enemy was still in the shadows: the wards slowly 'emptied', elective activities were interrupted, intensive care were freed up to create as many beds as possible.
"All this rapid transformation brought an atmosphere of silence and surreal emptiness to the corridors of the hospital that we did not yet understand, waiting for a war that was yet to begin and that many (including me) were not so sure would ever come with such ferocity.
"Cases are multiplying, we arrive at a rate of 15-20 admissions per day all for the same reason. The results of the swabs now come one after the other: positive, positive, positive. Suddenly the E.R. is collapsing.
"Someone already to be intubated and go to intensive care. For others it's too late... Every ventilator becomes like gold: those in operating theatres that have now suspended their non-urgent activity become intensive care places that did not exist before.”
ROME (Reuters) - A planeload of medical supplies, including masks and respirators, has arrived in Italy from China to help it deal with its growing coronavirus crisis.
The coronavirus outbreak began in China late last year but has since swept the globe. Italy is now the worst-affected nation in the world after China, with 1,016 dead and 15,113 confirmed cases since the contagion came to light there on Feb. 21.
A team of nine Chinese medical staff arrived late on Thursday with some 30 tonnes of equipment on a flight organised by the Chinese Red Cross.
"In this moment of great stress, of great difficulty, we are relieved to have this arrival of supplies. It is true that it will help only temporarily, but it is still important," said the head of the Italian Red Cross, Francesco Rocca.
"We have a desperate need for these masks right now. We need respirators that the Red Cross will donate to the government. This is for sure a really important donation for our country," Rocca said.
The outbreak risks overwhelming Italian hospitals and some key supplies are running low.
Below: A Chinese team of experts pose for a photograph with head of the Italian Red Cross Francesco Rocca after arriving at Rome’s Fiumicino airport on a chartered plane with a consignment of medical supplies including respirators and masks, to help Italy cope with a coronavirus outbreak, in Rome
In February 20, 2020, a patient in his 30s admitted to the intensive care unit (ICU) in Codogno Hospital (Lodi, Lombardy, Italy) tested positive for a new coronavirus, severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), the virus that causes coronavirus disease 2019 (COVID-19). He had a history of atypical pneumonia that was not responding to treatment, but he was not considered at risk for COVID-19 infection.1 The positive result was immediately reported to the Lombardy health care system and governmental offices. During the next 24 hours, the number of reported positive cases increased to 36. This situation was considered a serious development for several reasons: the patient (“patient 1”) was healthy and young; in less than 24 hours, 36 additional cases were identified, without links to patient 1 or previously identified positive cases already in the country; it was not possible to identify with certainty the source of transmission to patient 1 at the time; and, because patient 1 was in the ICU and there were already 36 cases by day 2, chances were that a cluster of unknown magnitude was present and additional spread was likely.
On February 21, an emergency task force was formed by the Government of Lombardy and local health authorities to lead the response to the outbreak. This Viewpoint provides a summary of the response of the COVID-19 Lombardy ICU network and a forecast of estimated ICU demand over the coming weeks (projected to March 20, 2020).
Setting the Priorities and the Initial Response
In Lombardy, the precrisis total ICU capacity was approximately 720 beds (2.9% of total hospital beds at a total of 74 hospitals); these ICUs usually have 85% to 90% occupancy during the winter months.
The mission of the COVID-19 Lombardy ICU Network was to coordinate the critical care response to the outbreak. Two top priorities were identified: increasing surge ICU capacity and implementing measures for containment.
Increasing ICU Surge Capacity
The recognition that this outbreak likely occurred via community spread suggested that a large number of COVID-19–positive patients were already present in the region. This prediction proved correct in the following days. Based on the assumption that secondary transmission was already occurring, and even with containment measures that health authorities were establishing, it was assumed that many new cases of COVID-19 would occur, possibly in the hundreds or thousands of individuals. Thus, assuming a 5% ICU admission rate,2 it would not have been feasible to allocate all critically ill patients to a single COVID-19 ICU. The decision was to cohort patients in 15 first-responder hub hospitals, chosen because they either had expertise in infectious disease or were part of the Venous-Venous ECMO Respiratory Failure Network (RESPIRA).3
The identified hospitals were requested to do the following.
Create cohort ICUs for COVID-19 patients (areas separated from the rest of the ICU beds to minimize risk of in-hospital transmission).
Organize a triage area where patients could receive mechanical ventilation if necessary in every hospital to support critically ill patients with suspected COVID-19 infection, pending the final result of diagnostic tests.
Establish local protocols for triage of patients with respiratory symptoms, to test them rapidly, and, depending on the diagnosis, to allocate them to the appropriate cohort.
Ensure that adequate personal protective equipment (PPE) for health personnel is available, with the organization of adequate supply and distribution along with adequate training of all personnel at risk of contagion.
Report every positive or suspected critically ill COVID-19 patient to the regional coordinating center.
In addition, to quickly make available ICU beds and available personnel, nonurgent procedures were canceled and another 200 ICU beds were made available and staffed in the following 10 days. In total, over the first 18 days, the network created 482 ICU beds ready for patients.
Containment Measures
Local health authorities established strong containment measures in the initial cluster by quarantine of several towns in an attempt to slow virus transmission. In the second week, other clusters emerged. During this time, the ICU network advised the government to put in place every measure, such as reinforcing public health measures of quarantine and self-isolation, to contain the virus.
ICU Admissions Over the First 2 Weeks
There was an immediate sharp increase in ICU admissions from day 1 to day 14. The increase was steady and consistent. Publicly available data indicate that ICU admissions (n = 556) represented 16% of all patients (n = 3420) who tested positive for COVID-19. As of March 7, the current total number of patients with COVID-19 occupying an ICU bed (n = 359) represents 16% of currently hospitalized patients with COVID-19 (n = 2217). All patients who appeared to have severe illness were admitted for hypoxic respiratory failure to the COVID-19 dedicated ICUs.
Surge ICU Capacity
Within 48 hours, ICU cohorts were formed in 15 hub hospitals totaling 130 COVID-19 ICU beds. By March 7, the total number of dedicated cohorted COVID-19 ICU beds was 482 (about 60% of the total preoutbreak ICU bed capacity), distributed among 55 hospitals. As of March 8, critically ill patients (initially COVID-19–negative patients) have been transferred to receptive ICUs outside the region via a national coordinating emergency office.
Forecasting ICU Demand Over the Next 2 Weeks
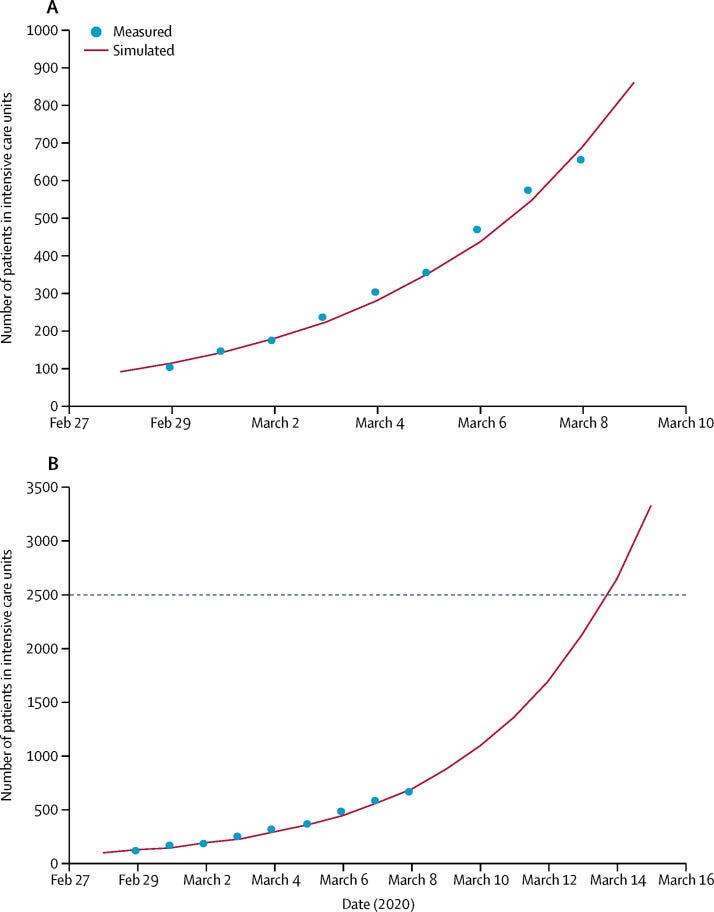
During the first 3 days of the outbreak, starting from February 22, the ICU admissions were 11, 15, and 20 in the COVID-19 Lombardy ICU Network. ICU admissions have increased continuously and exponentially over the first 2 weeks. Based on data to March 7, when 556 COVID-19–positive ICU patients had been admitted to hospitals over the previous 15 days, linear and exponential models were created to estimate further ICU demand (eFigure in the Supplement).
The linear model forecasts that approximately 869 ICU admissions could occur by March 20, 2020, whereas the exponential model growth projects that approximately 14 542 ICU admissions could occur by then. Even though these projections are hypothetical and involve various assumptions, any substantial increase in the number of critically ill patients would rapidly exceed total ICU capacity, without even considering other critical admissions, such as for trauma, stroke, and other emergencies.
In practice, the health care system cannot sustain an uncontrolled outbreak, and stronger containment measures are now the only realistic option to avoid the total collapse of the ICU system. For this reason, over the last 2 weeks, clinicians have continuously advised authorities to augment the containment measures.
To our knowledge, this is the first report of the consequences of the COVID-19 outbreak on critical care capacity outside China. Despite prompt response of the local and regional ICU network, health authorities, and the government to try to contain the initial cluster, the surge in patients requiring ICU admission has been overwhelming. The proportion of ICU admissions represents 12% of the total positive cases, and 16% of all hospitalized patients. This rate is higher than what was reported from China, where only 5% of patients who tested positive for COVID-19 required ICU admission.2,4 There could be different explanations. It is possible that criteria for ICU admission were different between the countries, but this seems unlikely. Another explanation is that the Italian population is different from the Chinese population, with predisposing factors such as race, age, and comorbidities.5
On March 8 and 9, planning for the next response, which includes defining a new hub and spoke system for time-dependent pathology, increasing ICU capacity further, and reinforcing stronger containment measurement in the community, has begun, as well as discussions of what could have been done differently.
First, laboratory capacity to test for SARS-CoV-2 should have been increased immediately. Laboratory capacity reached saturation very early. This can add extra stress to a system and affect the ability to make accurate diagnoses and allocate patients appropriately.
Second, in parallel to the surge ICU capacity response, a large, dedicated COVID-19 facility could have been converted more quickly. On day 1 of the crisis, it was not possible to predict the speed and extent of the contagion. Importantly, the forecasts show that increasing ICU capacity is simply not enough. More resources should be invested to contain the epidemic.
As of March 8, Lombardy was quarantined and strict self-isolation measures were instituted. This may be the only possible way to contain the spread of infection and allow resources to be developed for the time-dependent disease.
As of March 10, Italy has been quarantined and the government has instituted stronger containment measures, including strict self-isolation measures. These containment measures and individual citizen responsibility could slow down virus transmission.
While regional resources are currently at capacity, the central Italian government is providing additional resources, such as transfers of critically ill patients to other regions, emergency funding, personnel, and ICU equipment. The goal is to ensure that an ICU bed is available for every patient who requires one. Other health care systems should prepare for a massive increase in ICU demand during an uncontained outbreak of COVID-19. This experience would suggest that only an ICU network can provide the initial immediate surge response to allow every patient in need for an ICU bed to receive one. Health care systems not organized in collaborative emergency networks should work toward one now.
There is now grave concern regarding the Italian national health system's capacity to effectively respond to the needs of patients who are infected and require intensive care for SARS-CoV-2 pneumonia. The percentage of patients in intensive care reported daily in Italy between March 1 and March 11, 2020, has consistently been between 9% and 11% of patients who are actively infected. The number of patients infected since Feb 21 in Italy closely follows an exponential trend. If this trend continues for 1 more week, there will be 30 000 infected patients. Intensive care units will then be at maximum capacity; up to 4000 hospital beds will be needed by mid-April, 2020.
Italy has had 12 462 confirmed cases according to the Istituto Superiore di Sanità as of March 11, and 827 deaths. Only China has recorded more deaths due to this COVID-19 outbreak. The mean age of those who died in Italy was 81 years and more than two-thirds of these patients had diabetes, cardiovascular diseases, or cancer, or were former smokers.
Image above: “First patients of COVID-19 start to be taken in the new intensive care unit set up in a tensile structure at the San Raffaele hospital in Milan, Italy, Monday, March 23, 2020. For most people, the new coronavirus causes only mild or moderate symptoms. For some it can cause more severe illness, especially in older adults and people with existing health problems.”
Image above: “This picture taken on March 21, 2020 shows coffins on the ground of the church in Serina, near Bergamo, northern Italy. Italy on reported 793 new coronavirus deaths, a one-day record that saw the country's toll shoot up to 4,825, the 38.3 percent of the world's totality. The total number of fatalities in the northern Lombardy regions around Milan are more than 3,000.”
Overrun by critically ill coronavirus patients, Italy’s hospitals are choosing who gets lifesaving breathing machines and who does not.
It’s a scenario that could soon repeat in the United States, experts warn.
“The capacity in northern Italy hospitals is a preview of a movie that is about to play in the United States,” said Marty Makary, a Johns Hopkins University surgeon and health policy expert. “The best two indicators of what things will be like in the U.S. are the number of COVID-related deaths in Italy and the number of ICU beds.”
However, there are fewer than 100,000 ICU beds in the United States, according to a recent analysis by Johns Hopkins Center for Health Security.
Iran has become 'a tragic natural experiment' during coronavirus crisis
Hospitals in Italy and Iran are struggling to keep pace with round-the-clock demands of caring for a flood of patients, and both countries rank second and third, respectively, in total deaths.
Three weeks ago, Italy reported just seven deaths. By Tuesday night, more than 2,500 had died and the country was fast approaching the grim benchmark of more than 3,100 deaths in Wuhan and Hubei, China.
My comment: Among those who had been discarged alive or died in ICUs in Italy by March 25, 2020, the ratio was 256/405. That means 405 out of 661 died- 61.2%. 920 were still in the ICU alive.
Results: Among the 1581 patients with ICU disposition data available as of March 25, 2020, 920 patients (58% [95% CI, 56%-61%]) were still in the ICU, 256 (16% [95% CI, 14%-18%]) were discharged from the ICU, and 405 (26% [95% CI, 23%-28%]) had died in the ICU. Older patients (n = 786; age ≥64 years) had higher mortality than younger patients (n = 795; age ≤63 years) (36% vs 15%; difference, 21% [95% CI, 17%-26%]; P < .001).
A majority of patients in the Lombardy region of Italy with confirmed COVID-19 infection required mechanical ventilation, according to a paper published in JAMA.
Investigators from Italy retrospectively examined 1591 critically ill patients admitted to the hospital between Feb. 20 and March 18, 2020 in order to determine what were the baseline characteristics and outcomes of patients infected by the novel coronavirus and admitted to the intensive care unit (ICU). The first patient in Italy was diagnosed on Feb. 20 and brought to an ICU in Lombardy. A total of 17,713 people tested positive for COVID-19 through March 18 and of those, 9%, or 1591 patients, were admitted to the ICU. That was the group the study authors examined in their analysis. Most of the patients in the analysis were admitted to the ICU because of acute hypoxemic respiratory failure that required respiratory support, the study authors wrote.
For comparison, in China, the origin of the global outbreak, the percentage of patients with COVD-19 who required ICU care ranged from 5% to 32%, the investigators said.
A majority of the patients were male (82%), the study authors reported. The median age among patients was 63 years. The investigators classified patients as “younger” if they were 63 years old or less, and “older” if they were aged 64 or older.
Two-thirds of the patients had at least 1 comorbidity, most commonly hypertension (49% of patients with a comorbidity), the study authors found. Other comorbidities, such as cardiovascular disease and hypercholesterolemia were noted. A small group had a history of COPD. All of the patients aged 80 years or older had at least 1 comorbidity.
Almost all of the patients who had respiratory support data available and were admitted to the ICU needed invasive or noninvasive respiratory support: 1287 of 1300 patients, the study authors determined. A majority (88%) required endotracheal intubation and mechanical ventilation and the rest were treated with noninvasive ventilation.
Patients with hypertension were significantly older (66 years vs. 62 years) than their non-hypertension counterparts, the study authors said. The prevalence of hypertension was higher among patients who died in the ICU compared to those discharged from the ICU (63% vs. 40%, respectively), they added.
As of March 25, the investigators said that 58% of the patients in their analysis remained in intensive care, 16% had been discharged from the ICU, and 26% had died in the ICU. ICU mortality was higher in older patients and lower in younger patients and the percentage of patients discharged from the ICU was significantly higher among younger patients vs. older patients (21% vs. 11%, respectively).
The median length of stay in the ICU as of March 25 was 9 days, but ranged from 6 to 13 days, the study authors said. Among 920 patients that remined in the ICU on that date, the median length of stay was 10 days (8-14 days). For patients discharged from the ICU, the median length of stay was 8 days but among patients who died in the ICU the median length of stay was 7 days.
ROCCA DI PAPA, Italy (AP) — The World Health Organization has called it a “massacre.” The Health Ministry sent in inspectors. Prosecutors are investigating, and an appalled mayor said the managers of a residential facility she ordered sealed had “jeopardized the life and health of the most fragile.”
A scandal over coronavirus infections and deaths in Italy’s nursing homes took on broader dimensions Friday, with the National Institutes of Health conservatively estimating that at least 6,773 residents had died since Feb. 1, 40% of them either infected with the virus or with COVID-19 symptoms.
The true number is higher, since the agency surveyed a fraction of Italy’s eldercare homes and few residents of nursing homes nationwide were ever tested. But the institute’s survey gave a sample of the toll since Feb. 1: In hard-hit Bergamo province, 534 residents died. The province of Milan reported 749 deaths in nursing homes.
Some 36% of the thousands of deaths cited by the National Institutes of Health occurred in the second half of March, the period when infections were at their height in Italy and the country had the most virus-related deaths in the world.
The latest nursing home to be placed under police-enforced quarantine was in the tiny town of Rocca di Papa, in the hills south of Rome. Five people have died at the San Raffaele home and 148 tested positive for the virus, compared to 11 confirmed infections in the rest of the town.
“Inside it’s a ghost town,” recounted funeral home worker Luciano Bambino as he retrieved a body from the San Raffaele mortuary Friday. “The corridors, the gardens. It was deserted, spectral. They were all closed in, closed off from every point of view.”
The facility was cordoned off and its residents and staff placed in quarantine, after the acting mayor, Veronica Cimino, said the management failed to cooperate when she asked for data about virus prevention measures. Then, it was determined that the nursing home’s medical director lacked proper credentials for the job.
Prosecutors finally were called in to investigate after virus-related data and documentation didn’t line up, police said. Ambulances came and went Friday to transport critical patients to a hospital.
“It’s absurd that a private clinic has jeopardized the life and health of such fragile people,” Cimino told The Associated Press outside the facility. She said she was concerned for the residents inside and for their relatives, who have been prevented from visiting by government decree but also deprived of regular status updates from staff about the health of their loved ones.
The facility, for its part, blamed the region for failing to provide virus tests for residents and staff members, said it had recently replaced the medical director and stated it was cooperating with authorities to turn the home into a COVID-19 facility.
Criminal investigations of nursing home deaths and infections are underway elsewhere, including one targeting Italy’s largest care facility, the 1,000-bed Pio Albergo Trivulzio home in Milan.
Prosecutors got involved after staff reported that managers prevented them from wearing protective equipment and masks for fear of scaring the residents. The Trivulzio home has said it followed all security protocols.
The governor of the Lombardy region, Attilio Fontana, on Friday blamed unnamed “technicians” for a regional proposal he approved to send recovering COVID-19 patients to nursing homes to free up hospital beds. Unions representing medical workers have said the measure may have contributed to the infections at Trivulzio and elsewhere.
Fontana insisted he had done nothing wrong and noted that the transfers were only authorized if the nursing homes could guarantee isolated spaces and dedicated staff.
The Health Ministry launched its own investigation into the 143 Trivulzio deaths since March. It said it is seeking to determine if the hospital transfers violated ministry norms prohibiting the entry of possibly infected people into eldercare facilities .
This week, the World Health Organization representative advising the Italian government, Dr. Ranieri Guerra, termed Italy’s toll of nursing home deaths a “massacre.” He said the scandal must become an opportunity for the government to reassess how it cares for its elderly.
“I am part of an organization that is asking the government the same thing: What happened and why?” he said.
Relatives of residents want the same.
The newly constituted Justice and Truth Committee for the Trivulzio Victims, launched by the son of a Trivulzio resident issued a public demand for information and action to immediately protect residents.
“We want everything done to save our dear ones,” the group said in a statement.
As Italy prepares to emerge from the West’s first and most extensive coronavirus lockdown, it is increasingly clear that something went terribly wrong in Lombardy, the hardest-hit region in the country with Europe’s highest death toll.
Italy had the bad luck of being the first Western country to be slammed by the outbreak, and its official total of 26,000 fatalities lags behind only the U.S. in the global death toll. Italy’s first homegrown case was recorded Feb. 21, at a time when the World Health Organization was still insisting the virus was “containable” and not nearly as infectious as the flu.
But there also is evidence that demographics and healthcare deficiencies collided with political and business interests to expose Lombardy’s 10 million people to COVID-19 in ways unseen anywhere else, particularly the most vulnerable in nursing homes.
Virologists and epidemiologists say what went wrong there will be studied for years, given how the outbreak overwhelmed a medical system long considered one of Europe’s best, while in neighboring Veneto, the effect was significantly more controlled.
Prosecutors, meanwhile, are deciding whether to lay any criminal blame for the hundreds of dead in nursing homes, many of whom don’t even figure into Lombardy’s official death toll of 13,269, half of Italy’s total.
By contrast, Lombardy’s front-line doctors and nurses are being hailed as heroes for risking their lives to treat the sick under extraordinary levels of stress, exhaustion, isolation and fear. One WHO official said it was a “miracle” they had saved as many as they did.
Here’s a look at the perfect storm of what went wrong in Lombardy, based on interviews with doctors, union representatives, mayors and virologists, as well as reports from the Superior Institute of Health, national statistics agency ISTAT and the Organization for Economic Cooperation and Development, which advises developed economies on policy.
Caught unprepared
Italy was the first European country to halt all air traffic with China on Jan. 31, and it even put scanners in airports to check arrivals for fever. But by Jan. 31, it was already too late. Epidemiologists now say the virus had been circulating widely in Lombardy since early January, if not before.
Doctors treating pneumonia in January and February didn’t know it was the coronavirus because the symptoms were so similar and the virus was still believed to be largely confined to China. Even after Italy registered its first homegrown case Feb. 21, doctors didn’t understand the unusual way COVID-19 could present itself, with some patients experiencing a rapid decline in their ability to breathe.
“After a phase of stabilization, many deteriorated quickly. This was clinical information we didn’t have,” said Dr. Maurizio Marvisi, a pneumologist at a private clinic in hard-hit Cremona. “There was practically nothing in the medical literature.”
Because Lombardy’s intensive care units were already filling up within days of Italy’s first cases, many primary care physicians tried to treat and monitor patients at home. Some put them on supplemental oxygen, commonly used for home cases in Italy.
That strategy proved deadly, and many died at home or soon after hospitalization, having waited too long to call an ambulance.
Reliance on home care “will probably be the determining factor of why we have such a high mortality rate in Italy,” Marivi said.
Italy was forced to use home care in part because of its low ICU capacity: After years of budget cuts, Italy entered the crisis with 8.6 ICU beds per 100,000 people, well below the Organization for Economic Cooperation and Development’s average of 15.9 and a fraction of Germany’s 33.9, the group said.
As a result, primary care physicians became the front-line filter for virus patients, an army of mostly self-employed practitioners who work outside Italy’s regional hospital system.
Only those with strong symptoms were being tested because Lombardy’s labs couldn’t process more. As a result, these family doctors didn’t know whether they themselves were infected, much less their patients.
With so little clinical information available, doctors also had no guidelines on when to admit patients or refer them to specialists. And being outside the hospital system, they didn’t have the same access to protective masks and equipment.
“The region was extremely behind in giving us protective equipment, and it was inadequate because the first time, they gave us 10 surgical masks and gloves,” said Dr. Laura Turetta in the city of Varese. “Obviously, for our close contact with patients, it wasn’t the correct way to protect ourselves.”
The Lombardy doctors’ association issued a blistering letter April 7 to regional authorities listing seven “errors” in their handling of the crisis, key among them the lack of testing for medical personnel, the lack of protective equipment and the lack of data about the contagion.
The regional government and civil protection agency defended its efforts but acknowledged that Italy was dependent on imports and donations of protective equipment and simply didn’t have enough to go around.
Lost weeks
Two days after registering Italy’s first case in the province of Lodi, sparking a quarantine in 10 towns, another positive case was registered more than an hour’s drive away in Alzano in Bergamo province. Whereas the emergency room of the Lodi-area hospital was closed, the Alzano ER reopened after a few hours of cleaning, becoming a main source of contagion.
Internal documents cited by Italian newspapers indicate the handful of serious pneumonia cases the Alzano hospital saw as early as Feb. 12 were probably COVID-19. At the time, Italy’s health ministry recommended tests only for people who had been to China or been in contact with a suspected or confirmed positive case.
By March 2, the Superior Institute of Health recommended Alzano and nearby Nembro be sealed off as the towns in Lodi had been. But political authorities never implemented the quarantine recommendation there, allowing the infection to spread for a second week until all of the Lombardy region was locked down March 7.
“The army was there, prepared to do a total closure, and if it had been done immediately, maybe they could have stopped the contagion in the rest of Lombardy,” said Dr. Guido Marinoni, head of the association of doctors in Bergamo. “This wasn’t done, and they took softer measures in all of Lombardy, and this allowed for the spread.”
Asked why he didn’t seal off Bergamo sooner, Prime Minister Giuseppe Conte argued the regional government could have done so on its own. Lombardy’s governor, Atillio Fontana, shot back that any mistake ‘’was made by both. I don’t think that there was blame in this situation.”
Lombardy has one-sixth of Italy’s 60 million people and is the most densely populated region, home to the business capital in Milan and the country’s industrial heartland. Lombardy also has more people ages 65 and older than any other Italian region, as well as 20% of Italy’s nursing homes, a demographic time bomb for COVID-19 infections.
“Clearly, with the benefit of hindsight, we should have done a total shutdown in Lombardy, everyone at home and no one moves,” said Andrea Crisanti, a microbiologist and virologist advising the Veneto regional government. But he acknowledged how hard that was, given Lombardy’s outsize role in the Italian economy, which even before the pandemic was heading toward a recession.
“Probably for political reasons, it wasn’t done,” he told reporters.
Industrial lobbying
Unions and mayors of some of Lombardy’s hardest-hit cities now say the country’s main industrial lobby group, Confindustria, exerted enormous pressure to resist lockdowns and production shutdowns because the economic cost would be too great in a region responsible for 21% of Italy’s gross domestic product.
On Feb. 28, a week into the outbreak and well after more than 100 cases were registered in Bergamo, the province’s branch of Confindustria launched an English-language social media campaign, #BergamoIsRunning, to reassure clients. It insisted the outbreak was no worse than elsewhere, that the “misleading sensation” of its high number of infections was the result of aggressive testing, and that production in steel mills and other industries was unaffected.
Confindustria launched its own campaign in the larger Lombardy region, echoing that message, #YesWeWork. Milan’s mayor proclaimed that “Milan doesn’t stop.”
At the time, Confindustria Lombardy chief Marco Bonometti acknowledged the “drastic measures” needed in Lodi but sought to lower the sense of alarm.
“We have to let people know they can go back to life as it was, while safeguarding their health,” he said.
Even after Rome locked down all of Lombardy on March 7, it allowed factories to stay open, sparking strikes from workers worried their health was being sacrificed to keep Italy’s industrial engine rolling.
“It was a huge error. They should have taken the example where the first cluster was found,” said Giambattista Morali of the metalworkers’ union in the Bergamo town of Dalmine. “Keeping factories open didn’t help the situation; obviously, it worsened it.”
Eventually, all but essential production was shut down March 26. Confindustria’s national president, Carlo Bonomi, has been urging that industry be reopened, but in safe way.
“The paradigm has changed,” Bonomi said on RAI state television. “We can’t make Italians secure if we don’t reopen factories. But how do we make factories safe to secure Italians?”
It’s a tough sell, given that Lombardy is still adding an average of 950 infections daily, while other regions add from a few dozen to 500 each, with most new infections registered in nursing homes. Italy is set to begin a gradual reopening May 4, leading with regions farther south where the outbreak is more under control.
Lombardy probably will be last to fully open, with its 72,000 confirmed cases, 70% of Italy’s total, and estimates that the actual number could be 10 times that.
Costly field hospital
Perhaps no initiative better illustrates Italy’s confused coronavirus response than the 200-bed field hospital built in less than two weeks on the grounds of Milan’s convention center.
The hospital was unveiled to great fanfare on March 31, the fruit of a 21-million euro ($23-million) fundraising campaign headed by Lombardy’s governor, a member of the right-wing League party, to try to ease pressure on regional ICUs, which at that date were near capacity at 1,324 patients.
The national civil protection agency opposed the plan, arguing it could never equip it with ventilators or personnel in time. Instead, the agency, which reports to the rival 5-Star-Democratic government in Rome, preferred smaller field units set up outside hospitals and a program to move critically ill patients elsewhere.
In the end, the Milan field hospital was barely used, treating only a few dozen patients. Since it opened, Lombardy has seen pressure on its ICUs fall considerably, with slightly more than 700 people needing intensive care today.
Fontana, the governor, defended the decision and said he would do it again, telling Radio 24: “We had to ... prepare a dam in case the epidemic overcame the embankment.”
Nursing home ‘massacre’
While the regional government was focused on the field hospital and scrambling to find ICU beds, its testing capacity lagged, and Lombardy’s nursing homes were in many ways left to fend for themselves.
Hundreds of elderly have died in Lombardy and across Italy in what one WHO official has termed a “massacre” of those most vulnerable to the virus. Prosecutors are investigating dozens of nursing homes, as well as measures taken by local health authorities and the regional governments that may have worsened the problem.
Lombardy has more nursing homes than any other region, housing at least 24,000 elderly, and it registered more dead at those facilities than others too. Of the 3,045 deaths from Feb. 1 to April 15 in the region, 1,625 were either positive for the virus or showed its symptoms, according to preliminary results from a survey by the Superior Institute of Health.
Of particular attention to prosecutors was the March 8 decision by the regional government to allow recovering COVID-19 patients to be put in nursing homes to free up hospital beds. The region said it required the homes guarantee the patients would be isolated, but it’s not clear who was responsible to ensure that or whether anyone checked.
Even before that, staff at some homes said management prevented them from wearing masks for fear of scaring residents.
A March 30 regional decree, again aimed at easing pressure on Lombardy’s ICUs, told nursing home directors not to hospitalize sick residents 75 and older if they had other health problems. The decree said it was “opportune to treat them in the same facility to avoid further risks of decline in transport or during the wait in the emergency room.”
For the elderly at a nursing home in Nembro, one of the hardest-hit towns in Bergamo province, the decree amounted to a death warrant. But it wasn’t the first or only one that gave the home’s managers the sense that they were being abandoned.
When management proactively barred visitors Feb. 24 to try to guard residents and staff from infection, local health authorities responded by threatening sanctions and a loss of accreditation for cutting off family visits, said the facility’s new director, Valerio Poloni.
In the end, 37 of the 87 residents died in February and March. Its doctor, as well as Poloni’s predecessor as director, also tested positive, were hospitalized and died. A nursing home resident couldn’t get admitted to the hospital in late February because the ER was too crowded.
The nursing home’s health director, Barbara Codalli, said she was told to use her existing resources. “The patient returned a few hours later, and a few days later the patient died,” she told La7 television.
To date, none of the surviving residents has been tested. Poloni said tests were expected to begin in a few days. Two more residents died so far in April, but the situation seems under control.
“We are tranquil,” he said.
Associated Press staff writer Colleen Barry in Soave, Italy, contributed to this report
All COVID-19 patients (26/02/2020–18/04/2020) in the Rimini Province of Italy were included in this population-based cohort study. The hospitalized patients were classified according to the maximum level of respiratory support: oxygen supplementation (Oxygen group), non-invasive ventilation (NIV-only group), invasive mechanical ventilation (IMV-only group), and IMV after an NIV trial (IMV-after-NIV group). Sixty-day mortality risk was estimated with a Cox proportional hazard analysis adjusted by age, sex, and administration of steroids, canakinumab, and tocilizumab.
Results
We identified a total of 1,424 symptomatic patients: 520 (36.5%) were hospitalized, while 904 (63.5%) were treated at home with no 60-day deaths. Based on the respiratory support, 408 (78.5%) were assigned to the Oxygen group, 46 (8.8%) to the NIV-only group, 25 (4.8%) to the IMV-after-NIV group, and 41 (7.9%) to the IMV-only group. There was no significant difference in the PaO2/FiO2 at IMV inception in the IMV-after-NIV and IMV-only groups (p=0.9). Overall 60-day mortality was 24.2% (Oxygen: 23.0%; NIV-only: 19.6%; IMV-after-NIV: 32.0%; IMV-only: 36.6%; p=0.165). Compared with the Oxygen group, the adjusted 60-day mortality risk significantly increased in the IMV-after-NIV (HR 2.776; p=0.024) and IMV-only groups (HR 2.966; p=0.001).
The present study showed how an integrated multidisciplinary clinical organization was able to optimize the allocation of the available resources among 520 hospitalized COVID-19 patients. The overall 30- and 60-day mortality were 22.5% and 24.2%, respectively. Approximately 21% of the patients were mechanically ventilated, with a mortality ranging from 19.6% in the patients treated with NIV-only to 36.6% in the patients undergoing IMV without an NIV trial. To our knowledge, this is the first study reporting 60-day mortality in a cohort of hospitalized patients diagnosed with COVID-19 overall and according to all adopted ventilatory strategies. A Chinese multicentric study enrolling 258 ICU patients reported an overall 60-day mortality of 64.3%, with 19 patients deceased within 48h after ICU admission.19Among 165 mechanically ventilated patients, the 60-day mortality was 83%, 56%, and 94% for those treated with IMV, with NIV, and receiving both treatments, respectively. The median P/F ratio in the Chinese population was 91 (IQR 67–134) with a SOFA score of 6 (IQR 5–7). It should be noted that, in our study, we documented results for patients treated with NIV and/or IMV despite a similar P/F ratio (median 98.0; IQR 84.0–124.5) and a higher SOFA score (median 8; IQR 6–10), with a considerably lower 60-day mortality rate overall and in individual groups.
Of the 1591 patients included in the study, the median (IQR) age was 63 (56-70) years and 1304 (82%) were male. Of the 1043 patients with available data, 709 (68%) had at least 1 comorbidity and 509 (49%) had hypertension. Among 1300 patients with available respiratory support data, 1287 (99% [95% CI, 98%-99%]) needed respiratory support, including 1150 (88% [95% CI, 87%-90%]) who received mechanical ventilation and 137 (11% [95% CI, 9%-12%]) who received noninvasive ventilation.
Italy was the first western country facing an outbreak of coronavirus disease 2019 (COVID-19).1 The first Italian patient diagnosed with COVID-19 was admitted, on Feb. 20, 2020, to the intensive care unit (ICU) in Codogno Hospital (Lodi, Lombardy, Italy), and the number of reported positive cases increased to 36 in the next 24 hours, and then exponentially for 18 days. This triggered a prompt, coordinated response of the ICUs in the epicenter region of the outbreak that resulted in a massive surge in the ICU bed capacity.2
An Italian registry from 3 northern Italian regions (Lombardy, Emilia-Romagna and Veneto) showed that the rate of ICU admission was 12.6% of COVID-19 hospital admissions. Eight hundred and five patients were admitted and treated in the ICU among 6378 patients hospitalized for COVID-19 in the period between Feb. 24 through March 8, 2020.3 The coordination of a critical care response in Italy happened in collaboration with out-of-hospital, and out-of-ICU management of patients with respiratory failure.
Through a central coordination of the ICU Network, 130 ICU beds dedicated to COVID-19 patients were created in Lombardy in 48 hours. After the saturation of the designated hub hospitals, almost all hospitals of the region created dedicated ICUs, and on April 2, the ICU capacity reached 1750 beds. In addition, on March 31, 2020, the Milan Fair COVID-19 Intensive Care Hospital was inaugurated. The project, developed by Fondazione Fiera Milano in partnership with Lombardy Region consisted of a temporary hospital with up to 250 ICU beds developed in 20 days, and covering more than 25,000 square meters (Fig. 1 ). The hospital reorganization process, with the opening of newly dedicated ICUs, has been a multidisciplinary effort, with the involvement of health care providers, hospital managers, and political authorities.7, 8, 9The Italian government allocated 845 million euros to the National Health System to ensure a progressive increase of the number of ICU beds for invasive mechanical ventilation, up to 14% of the total hospital beds.10
END
C’s Newsletter is a reader-supported publication. To receive new posts and support my work, consider becoming a free or paid subscriber.
"If the PCR tests came back positive, medical professionals killed their patients with protocols, simple as that. They don’t think for themselves. They follow orders. Even if they observe deaths over and over from their “treatments,” they don’t care. If their jobs depend on killing, they kill."
Most microbiological (virological) scientists are from the biotechnology industry, and will always have multiple conflicts of interest and therefore won't want be able to have honest, critical viewpoints or even be able see one in the first place.
However, most regular industry insiders will remain agnostic to all of what's happening, either out of choice or from lack of a critical awareness, and so will likely work to bolster the PCR and LFTs or any such biotech products.
Because of the science veneer of these technologies, and those proposing them; most clinicians become assuaged by the seemingly impressive performative aspects of these technologies and thereby become more convinced of their worth over and above their own diagnostic judgments.
They are also "required" via administrative diktats that come from on high to "follow the rules" as prescribed by those who initiate use of these tests and then mandate deadly protocols based on said fraudulent results of the tests.
What has happened to humanity have we all not watched the Holocaust movie and see the same pattern to exterminate the innocent ! There are serious psychopaths running the world, and they will not stop until they kill all of us!












"If the PCR tests came back positive, medical professionals killed their patients with protocols, simple as that. They don’t think for themselves. They follow orders. Even if they observe deaths over and over from their “treatments,” they don’t care. If their jobs depend on killing, they kill."
There it is right there folks.
Two articles on Italy re: covid con:
https://healthfreedomdefense.org/italy-2020-inside-covids-ground-zero-was-there-really-a-pandemic/
https://healthfreedomdefense.org/italy-2020-the-preposterous-pandemic/
A snippet from a comment I made today:
Most microbiological (virological) scientists are from the biotechnology industry, and will always have multiple conflicts of interest and therefore won't want be able to have honest, critical viewpoints or even be able see one in the first place.
However, most regular industry insiders will remain agnostic to all of what's happening, either out of choice or from lack of a critical awareness, and so will likely work to bolster the PCR and LFTs or any such biotech products.
Because of the science veneer of these technologies, and those proposing them; most clinicians become assuaged by the seemingly impressive performative aspects of these technologies and thereby become more convinced of their worth over and above their own diagnostic judgments.
They are also "required" via administrative diktats that come from on high to "follow the rules" as prescribed by those who initiate use of these tests and then mandate deadly protocols based on said fraudulent results of the tests.
https://sanityunleashed.substack.com/p/false-positive-pcr-driven-pseudo/comment/63494666
What has happened to humanity have we all not watched the Holocaust movie and see the same pattern to exterminate the innocent ! There are serious psychopaths running the world, and they will not stop until they kill all of us!