


On Milk and Cows, COVID and Ivermectin, and why Robert Malone doesn’t need to stay “confounded” forever

I was looking at a LIMDEP tutorial on youtube recently to see if it had changed much since the last time I used it over a decade ago. (It hasn’t). The example data set that they were using took me back a bit to my college days. I want to keep making this point until people get it: Medical intelligence has been retarded through clinical trial modeling.
I use the word “retarded” in the sense of “held back.” Robert Malone and others in the field of medicine are very intelligent individuals. The reason why they continue to avoid using the correct methodology to cure disease and answer their questions about medicine is unclear to me at the moment. I’ve been making this point for some time now.
And I will be specific on some things that Robert Malone has said, to highlight the problem, with all due respect to him, because if I can just get the medical community to understand the problem and the solution, they could save millions of lives. I’m not trying to make this personal.
Anyway, on to the example. They were using some variable in LIMDEP that took me back.
Cows and Milk.
Anyone can think of several factors that influence the production of milk. Just like anyone can think of several factors that influence “COVID” death rates. Can you isolate and quantify all these individual factors in the real world, while they are all mixed together? Yes. Does the medical community do that? No.

Agriculture is a good example of an application of "econometrics." This type of math, multiple linear regression using ordinary least squares, is often used in economics, so that's where "econometrics" gets its name. If you want to know how interest rates influence GDP, you can't conduct a controlled trial of the entire economy in a lab. That's not necessary though. You can just analyze the real world. You can use econometrics for anything though.
It reminds me of where I learned econometrics, Auburn University. Auburn is also well-known for their college of Agriculture. Agriculture is a major and common application of econometrics. The first class I took on econometrics was called Introduction to Agricultural Econometrics, in Fall 2001. I still remember that class because that was where I first heard about 9/11. Everybody remembers where they were when they heard. I was in class. The Professor was late coming into the classroom, and then he came in and told us.
Is there an equivalent course Introduction to Medicinal Econometrics? There was, once. It was at the London School of Hygiene and Tropical Medicine, Introduction to Medical Statistics. LSHTM is closely associated with the WHO today. LSHTM used econometrics to identify and quantify factors that caused death in a population. This is an important fact for several reasons and I intend to expand on it in another article. The point here is that the reader should naturally ask "if this works so well why doesn't the medical community do it?" I asked the same question. They did it, then it disappeared from use in the medical community for the most part as far as I can tell. Notice the shrinking text of the textbook. It basically means that they knew how to find and quantify variables that caused increased mortality in my opinion. Thomas Malthus was British as well, and was the first to publish theories supporting "population control."

So let’s say that you want to know how inputs affect the production of milk. Let’s keep it simple. I’m not a farmer, but bear with me. Our variables are Milk, Cows, Land, Labor. The amount of milk produced is determined by the number of cows, the amount of land, and the amount of labor. Milk = Cows + Land + Labor. Milk is the dependent variable; the others are independent variables. Milk depends on the amount of land each cow has to graze on, the number of cattle, the amount of time you spend milking them, in my oversimplified farm. Not complicated.
I would import raw data from an excel spreadsheet. Variables are in columns. The rows are “observations." In this case the observations are years. Each year, the farm has a different mix of cows, land, and labor, and the farm produces a different amount of milk. Import the data into LIMDEP. The left hand side variable = Milk. The right hand side variables are the others. Regress.

That’s it. Done. (That's not the regression they ran above). I don't know what the variable Y/T is. I didn't listen.
Now you know how much each independent variable affects the dependent variable. You don't need to conduct and experiment, hold every independent variable constant, except one which you adjust to see the effect. Frederick Gauss said it was his gift to the world useful in all application of science. The globalist Malthusian death cult kept it for themselves and hid it from the rest of the medical community.
Of course you can make models more complicated. I went to school with someone who was going to work for a company that raised fish in cages. To optimize that business for profit, he was to regress the amount of food, the type of food, water conditions, and so on, against output. Then you can put the information gained into a profit maximization formula, because the prices of all inputs and outputs are always changing.
Now let’s talk about medicine today.
Dr. Robert Malone is a very highly regarded man among his peers. As Stew Peters said on January 22, 2022: “One day after being banned, Malone went on the Joe Rogan show, and he asked a very relevant question: “If I'm not qualified to talk about this, who is?’”
In my opinion, Robert Malone is an expert on a few things. 1. How to trick your cells into accepting manufactured mRNA that they would otherwise reject. 2. How the vaccine approval process works, how to get papers published, how to get funding, and other the behind-the-scenes stuff.
On August 29, 2021, Dr. Robert Malone noted the sharply lower rate death rates in nations in Africa in countries that used Ivermectin more heavily than other nations in Africa in the period coinciding from roughly March 2020 to August 2021. “Well, what a strange coincidence…” Malone wrote on Twitter.

I thought that was an extremely important observation. Why weren’t people dying in Central Africa? Malone had implied that maybe Ivermectin use was the difference. The African nations with the lower "COVID" death rates also used more Ivermectin than other African nations to prevent “river blindness” caused by the larvae of flies.
Then the next day, August 30, Malone walked back his Ivermectin theory a bit, because he had discovered that obesity was another identified factor in "COVID" death rates: “DEATHS/100K in African Countries: Obesity or Ivermectin? Science- is all about pattern recognition, then finding more patterns - generating alternative hypothesis. This is what good scientists do. They 'listen' to the data. This is what Jill discovered this morning.”

I thought, "'listen', to the data," what does that even mean? And I replied to the gentleman, “This is what regression analysis could answer. Obesity and literacy every other factor you can quantify. One equation simultaneously. The more factors, the stronger the model.”

On August 30, the same day that I essentially told Malone that regression analysis could handle multiple variables, someone else brought up another variable that could potentially explain the lower “COVID” death rates in Africa. This variable was pre-exposure to malaria. Some immunity from Malaria could possibly carry over to “COVID.” Malone replied to this account, but not to me.

Malone replied: “analysis of epidemiological data is really hard to get right now due to confounding and masking. It is so, so easy to fall in love with your favorite hypothesis and overlook alternate hypotheses. Confounding variables are everywhere. Reason why prospective randomized trials are done.”
He called these factors “confounding variables” and said it was the reason why the medical community did randomized trials.
And I’m thinking, Robert Malone does not need to be “confounded.” I had never heard the term “confounding variables” in school. These are called “independent variables.” Since Malone would not reply to me on twitter, and it was clear to me that the medical community was ignorant of the staggeringly superior methodology of multivariate regression, or at least that it was not practiced by medical “experts,” I figured that I should write something more detailed for Malone to read in a polite and professional manner. By that point, Malone had said that he was a voracious reader of all papers related to COVID. He still says that.
So I did that.
I wrote “Hypothesis for Dr. Robert Malone.” I published in September 04, 2021. I put it on his twitter page and asked him to comment. Didn’t happen. Maybe I didn't have the necessary "credentials," to suit him, or I wasn't a "peer"- or maybe he just didn't want to talk about it. (He would also later not respond to other things I asked him about on the report of Jiang and Mei about the genetic damage caused by the mRNA injections that would likely (and did) lead to greatly increased cancer rates, and the use of graphene as a delivery method for mRNA.
In "Hypothesis for Dr. Robert Malone," to highlight the statistical methodology I was attempting to explain, I took an issue Malone had raised around the same time as he did Ivermectin and Africa - fructose and obesity. Fructose consumption and obesity are correlated of course. The implication here, the way I saw it, was that “obesity” per se may not have been the factor that led to higher “COVID” death rates - fructose could have been it.
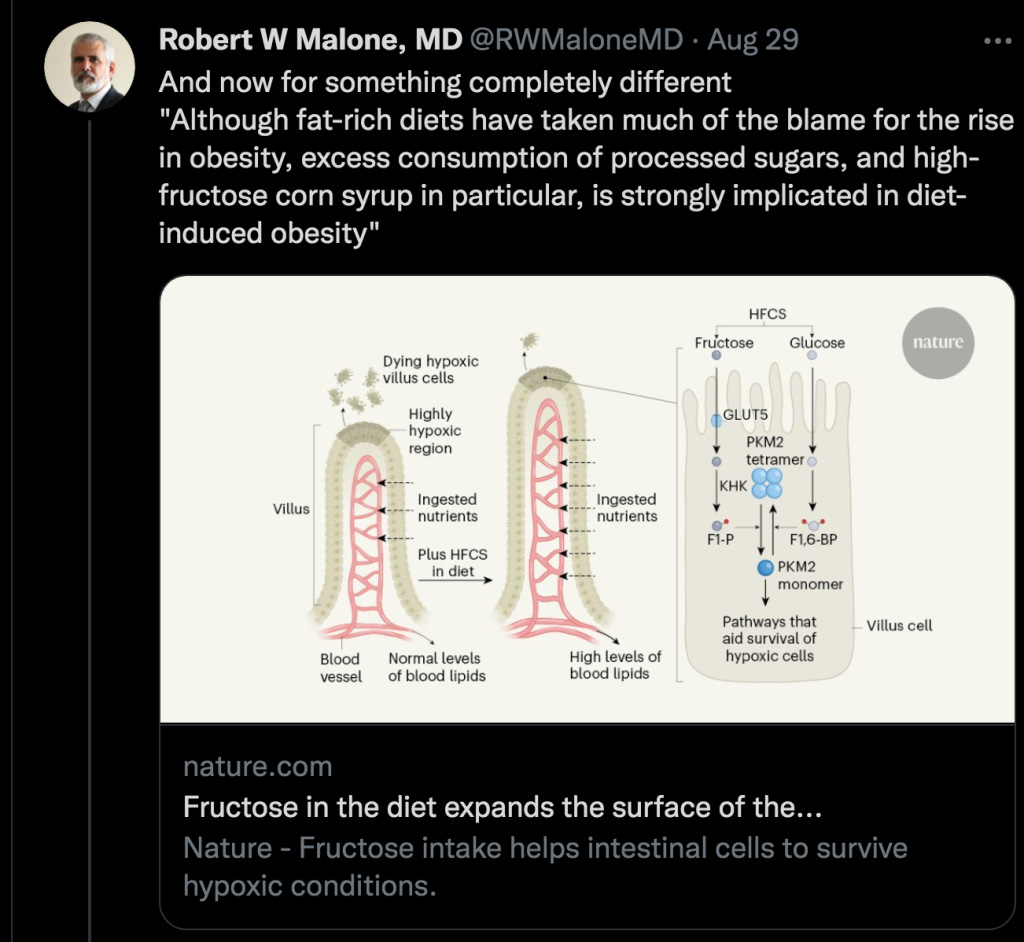
There’s more than one way to become obese. In a regression, you can use both body mass index (BMI) and fructose consumption as independent variables (provided that the two variables aren’t too highly correlated with each other. If the two variables are too highly correlated with each other, that creates a problem called “multicollinearity.” I wouldn't use both GDP and GNP as independent variables when modeling the stock market, for example. It makes the conclusions of the regression invalid. There are rules for this. It’s simple to check for multicollinearity before running a regression though, and I doubt they are overly correlated).
Assuming obesity and fructose consumption are not too highly correlated, you can test the hypothesis that there is some problem on the cellular level caused by fructose that is independent of BMI per se. Breaking apart fructose and BMI in multivariate regression was the issue was that I highlighted to help Malone understand the multivariate regression methods and applications to answer his questions and theories.
Anyway, my efforts with him were a waste of time, but maybe not with the rest of you. Let's get back to "COVID" death rates and Africa. Here’s how to answer the question of why some countries were dying at higher rates than others. Before I start, I need to point out that "theory" is important. Very important. You have to put the proper variables in the model, or your conclusions are crap. That was drummed into our heads in college. To not use "theory" was to data mine. Data mining was frowned upon greatly.
And there's a very good reason for that, because if you leave out a true explanatory variable according to theory, you can still find all types of correlations. Some may be "spurious correlations," as they are called, if you do not include the true cause. Someone had once demonstrated that the menstrual cycle of a blue what were correlated with economic cycles. That was the humorous example that we were given about spurious correlation.
Let me give some background on my theories about "COVID." I'm not a virologist, a microbiologist, an MD or anything like that. I learned as I went and I'm still learning. The whole point of this is not to try and find the answers for you according to medical theory, but to explain to the reader the correct method to answer the questions. It is not the randomized control trials as described by Robert Malone.
By the way, we were also told to publish the original data set along with our methodology. If you didn't publish the data, who could say that you didn't just make up the conclusions? Like anyone would ever do that, we thought. In every "COVID" or Vax stat I've ever seen I have never found a link to the original data so that I could analyze it myself. That's one of the ways I knew they were all lying.
Back to the point on "COVID" theory, after I wrote the Hypothesis for Dr. Malone, I set out to research the use of Ivermectin in Africa and how it may have affected COVID death rates, because I thought it made sense. On December 28, 2021, I published “Nigeria never got COVID because Nigeria was using Ivermectin.”
Back then, I was under the impression that most people are under today, that the “Pandemic” was driven by a virus that spread from person to person. I haven’t dismissed that as a possibility completely yet, but I’ve seen plenty of reasons to question it a great deal. I'll get to those, and how I would set about answering my questions.
In this time period, late 2021, at my information level, I reasoned that Ivermectin use acted as some sort of firewall to prevent COVID from spreading. That's what Malone had originally implied before he quickly backed off due to the other "confounding" variables. Nigeria used Ivermectin more than any other nation. Nigeria had very good doctors who had submitted a report to the WHO on the positive effects of Ivermectin on "COVID." They spurned the vaccines. COVID passed over Nigeria like the death angel passed over homes with the blood of lambs painted over the doors. I wrote about it. I figured it was Ivermectin.
Here’s what I think happened now. Call it a hypothesis. The vaccines killed people in the period from December 2020 - present. These deaths are falsely associated with “COVID” that was caused by a virus. Whether or not a PCR test comes back positive for a virus fragment replicated many times over does not mean that the virus fragment was the cause of a given death or disease. Kary Mullis spoke about this spurious correlation extensively with PCR tests, HIV, and AIDS.
In the period from roughly March 2020 - December 2020, there was little or no excess death from “COVID,” I think. It was just a false association. In this period, I expect to see "COVID death" correlated with "PCR tests," and I expect the rest of the explanatory variables be largely insignificant. Not that the other variables can't have good effects in a lab, mind you, but if people aren't dying from a virus, then these variables aren't protecting you from dying from that virus either.
Note that some people believe that 5G can be used to simulate disease symptoms and cause death and that could have been used to simulate the spread of a disease. I don’t know how to create a variable for someone manipulating direct energy for a sinister purpose though. I still think the data will tell us a great deal even if that happened.
In the period December 2020 - present, vaccines took over from PCR tests as the primary cause of death. There is no doubt about this part in medical theory today. If you don't accept that the "vaccines" are unsafe and counter-effective at this point, you simply have no credibility, regardless of your credentials and how much you deny the obvious.
In fact, the death cult at the WHO, with the most advanced surveillance and statistical methodology in the world, went on a crusade to cause death in the African nations that were not vaccinating their populations to death. They decried what they called "vaccine inequity." Maria Van Kerkhove, who received her Ph.D. in epidemiology from the London School of Hygiene and Tropical Medicine, of course, gave a freaking lecture where she had a graph of the lower vaccination rates in these African countries. These African countries were so poor, you understand, that you needed to give them money to buy vaccines and kill their people.

Of course the WHO knew damned good and well that these same African nations with lower vaccination rates also had lower "COVID" death rates - from their own data in the WHO.
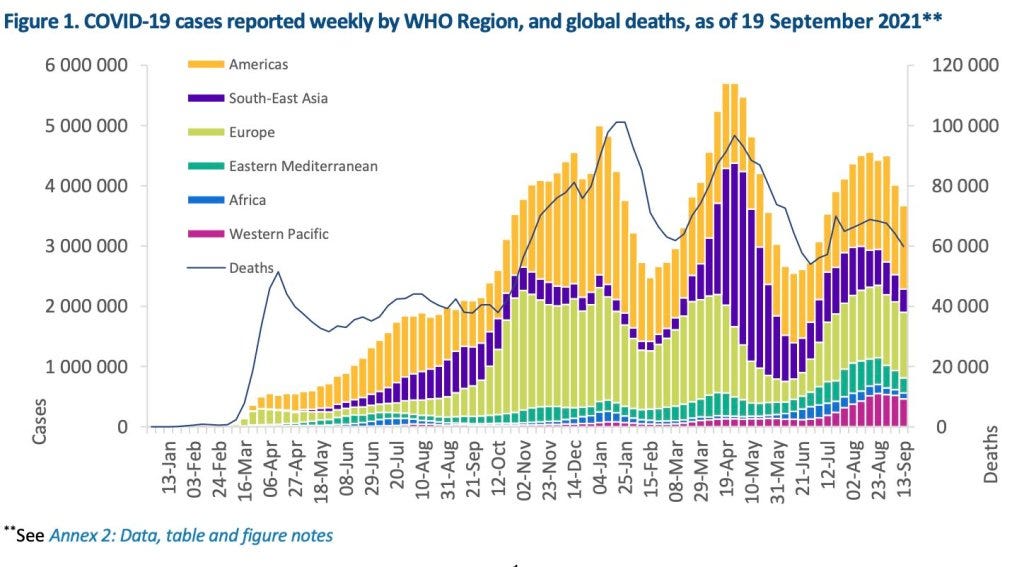
So anyway, here is how I would run a model. COVID Death Rate = COVID Test Rate + Vaccine Rate +Sunlight Exposure + Malaria Exposure + Body Mass Index + Ivermectin Rate.
I think if it is done in the periods I mentioned, with good data sets, it should tell us a great deal.
If you think the model is insufficient, you can criticize it. For instance, some of you may have thought earlier that "water" or "rainfall" should have been included in the farm model. Water grows the grass on the land that the cows eat to make milk. Assimilate, learn. Just get the data and run it again. Add a column, click. I only want to know the truth.
So that should give you an idea how it works.
I finished my Hypothesis to Dr. Malone with the words of Friedrich Gauss, who called this method "the most fruitful in every application ... to natural philosophy."

But the medical community won't listen, not yet anyway. If it was up to Robert Malone, they'd do a controlled experiment with all of the above variables, one variable a time, while holding the rest constant, to find individual correlations in a laboratory setting. And that could not possibly tell you what actually happened in the real world with all the variables combined. The question is not what could have potentially happened, but what did happen.
Charles Wright